Story Telling Problem Based Learning (ST-PBL): A Program for Rural Elderly with Chronic Diseases
Article information
Abstract
Purpose
To measure changes in health knowledge, health attitudes, and health promotion behaviors of the elderly in rural communities after using the Story Telling Problem Based Learning program facilitated by students in a nursing course.
Methods
A quasi-experimental study using a non-equivalent control group: 72 students sampled from the nursing discipline were divided into experimental (n=36) and control groups (n=36). The ST-PBL program was provided to the older rural people in the experimental group for six weeks.
Results
Data were analyzed using the SPSS/WIN 21.0. After the application of the ST-PBL program, the participants in the experimental group showed a significant increase in health knowledge and health promotion behavior.
Conclusion
The participants in the experimental group demonstrated positive changes in health knowledge, health attitudes, and health promotion behaviours. The use of an approach such as the ST-PBL program can promote uptake of self-care behaviors within the elderly with chronic diseases living in rural areas.
INTRODUCTION
In 2020, older people in Korea accounted for 16.4% of the total population, and now the country is considered an aging society. The elderly population living in rural areas accounts for 16% to 22% of the total resident population, and rural areas often have the status of a super-aging society (Statistics Office, 2020).
As the elderly population grows, it faces several problems. The biggest problem is that most older individuals have chronic diseases. In 2017, the proportion of older people with three or more chronic diseases increased by 20.3% from 51% in 2008, which means that the age of longevity with prevalence of disease is approaching (Statistics Office, 2018). Therefore, appropriate preventive care is as important as treating disease of the elderly in contemporary communities (Yoon, 2017). Problems that arise from chronic diseases in the elderly include physical problems such as discomfort, pain, and dysfunction. In addition, various problems, particularly psychological problems (loss of self-esteem, depression, and stress) and economic difficulties, such as social isolation and weakening of social support, have appeared (Choi, 2012). Therefore, it is necessary to support chronically ill elderly patients in an integrated manner because they must deal with not only physical and emotional problems, but also focus on the issues around social support difficulties. However, until now, the development of a program which not only follows the PBL philosophy but also actively integrates all aspects of the management of chronic diseases in the elderly had not been created.
The first problem with the management of chronically ill elderly living in rural areas is that systems for patients to actively participate in their treatment have not been not well established. For example, in terms of chronic diseases, the rate of completion of hypertension management education in rural areas was 11.1%, which is below the national figure of 19.4%. In addition, the rate of completion of diabetes management education is 26.5% nationwide, but 16.3% in rural areas, and while there is 16.5% of arthritis management completion rates nationwide, it is significantly lower in rural areas at 3.6% (Korean Center for Disease Control, 2019). The second problem is that the practice rate of daily life health management is low. To minimize the impact of chronic disease, preventive strategies in addition to self-care in daily life are important. When necessary, acute care treatment is available, however the systematized self-care strategies are important and should be continued to the patient’s ability. Essential elements for health such as rates of smoking cessation, alcohol consumption, and physical activity, are lower in rural compared to other regions. Smoking in rural areas was 21.8% but 20.1% nationwide; the drinking rate was 60.7%, and 57.3% nationwide, and the rural walking practice rate was 29.6%, lower than the nationwide rate of 39.5% (Korean Center for Disease Control, 2019). One of the goals to be achieved in the National Health Promotion Comprehensive Plan is to bridge the gap between regions and offer population health support nationwide which is adapted to each of the differing needs of the lifestyles in the urban and rural regions.
Park et al (2018) argued that a nursing approach is needed to solve the problems that are present to reduce the health gap between regions. By identifying the reasons for the attrition in programs addressing daily life health practices with respect to chronic diseases occurring in rural communities, the project team suggested approaches to improve chronic disease management that were outside of the usual educational approach and material and then to verify the effectiveness of a program consistent with PBL methodology; more person-centered, involving collaboration between educational providers and the older people using their real-life problems as stimulus for learning about preventive healthcare strategies.
According to the National Assessment of Literacy Survey in the United States, only 3% of the elderly population had adequate health literacy (Speros, 2011). In Korea, approximately 42.8% of older people with a disability, understand and use health information (Lee & Kang, 2008), and the level of literacy on elderly health is relatively low (Park & June, 2011). Therefore, to provide health information for rural seniors, there is an urgent need to develop suitable education programs. However, publicly available information on the use of healthcare is often difficult to understand: It is written in a complex manner making it difficult for the elderly creating barriers to use of self-care strategies to address problems (Lee & Park, 2010). Without considering the appropriate educational approach for the elderly, educational materials are generally considered ineffective (Lee, 2018).
The storytelling learning method is a suitable pedagogical method for the elderly because they experience memory loss due to aging or difficulty in physical functioning and in accepting and using new things in life (Gee, 2013). Storytelling or “the act of telling a story” (Ahn, et al, 2013) can be used as a critical alternative to the traditional learning methods in various subjects and contemporary education programs (Eagon, 2005). Storytelling is a motivational approach that captures the desire for memorable moments in learning, helps the learners with recall of stories, and has a great educational effect on replay (Lee, 2008). Vivian (2009) explained that intentional storytelling works because it brings fact-based information along with emotion-based human interest, and that these emotions play an important role in our ability to understand new thoughts. Using storytelling, simple stories provide stimuli for learning and this helps in the process of finding various problems in the story and the storyteller finding answers themselves. In this way customized educational programs tailored to the elderly can be offered. In addition, through this approach, storytelling about a health-related problem based on a classic story that many elderly people have encountered. It is an educational approach that accurately reflects the characteristics of the elderly who are planning to proceed to finding answers that meet their own needs. Following the development of a ST-PBL program to improve the health promotion ability of the elderly with chronic diseases living in rural areas, the authors were keen to examine the nature and extent of the older persons’:
1) Health knowledge about their own needs
2) Attitudes to addressing health problems
3) Health promotion behavior that was new to them.
METHODS
Conceptual framework
The conceptual framework of this study was used in previous research by Wan et al. (2016). The framework consisted of the knowledge, attitude, practice-performance model (knowledge, attitude, practice-outcome model, KAP-O model) (Figure 1).

Conceptual framework.
Program setting and participants
Chronic disease refers to health breakdown where physiological function gradually declines and degenerates and causes disorders that increase demand for services characterized by rehabilitation therapies and continuous supervision, observation for the emergence of health deterioration, and nursing intervention (Shin et al, 2019).
In this study, only hypertension, diabetes, and hyperlipidemia were included in our use of the Korean National Health and Nutrition Examination Survey (KNHANES). The subjects were elderly people aged 65 and over, who lived in rural areas where their diagnosis of chronic diseases had taken place more than 1 year previously.
Program composition and progress conceptual framework
To develop the educational program of this study, the intervention mapping protocol (IMP) method by Bartholomew et al. (2016) was applied as shown in Figure 2.
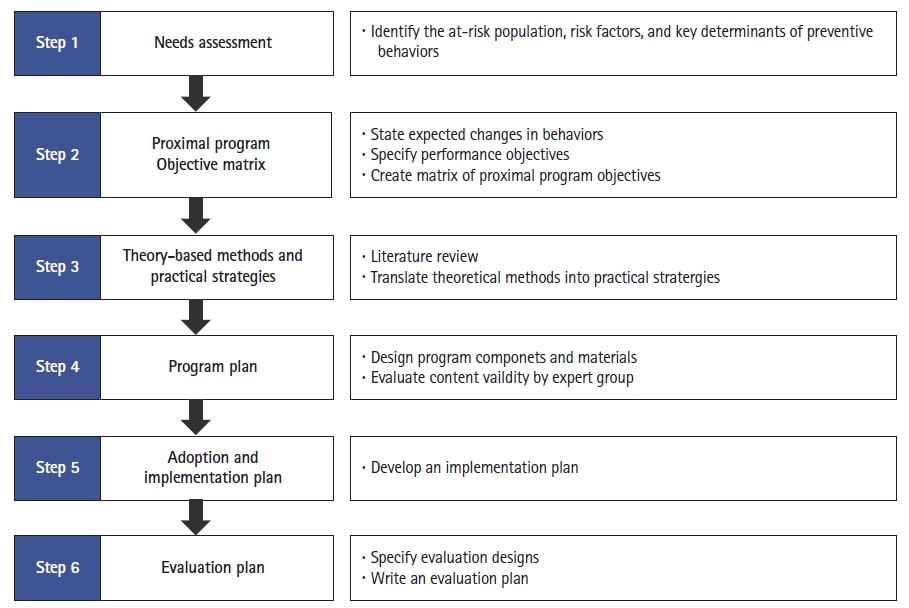
Program composition and progress.
Step 1: Needs assessment
Specification of the health-related problems and who needs to change as the focus for the project. Confirmation of the issues and needs assessment took place through a literature review, questionnaire survey, and interviews. The literature review provided evidence of educational levels of education as one reason for difficulty in managing chronic diseases among older people living in rural communities. Feedback from interviews and surveys with elderly residents in the community, supported the need for education but also found that the content of existing educational offerings was difficult and boring.
Step 2: Proximal program objective matrix
Goal setting is the process of subdividing performance goals by describing the outcomes expected to be achieved through mediation. The most important issue identified was to induce changes in behavior by changing attitudes informed by knowledge. To induce behavioral change, a program was constructed to develop a positive attitude by providing basic knowledge about chronic disease and ways to manage symptoms. The degree of achievement of the goal was measured the end of the program.
Step 3: Theory-based methods and practical strategies
In this step, the process of selecting theories was applied to achieve behavioral change, by turning theoretical concepts into actionable activities. It was constructed based on the KAP-O model to change the health promotion behavior of the elderly living in the community. In the KAP-O model, the ST-PBL program needs to provide the necessary information and motivation for changes in behavioral skills. Unlike existing educational programs, this ST-PBL program has a strategy that can be easily accessed by storytelling, through the classic Korean novels (Heungbu & Nolbu and Kongjwi Patjwi, Simcheongjeon). It is a novel that is easy for the elderly to understand, and through its use, the elderly can learn about health-related knowledge and use it to develop a positive attitude to preventive health behaviors.
Step 4: Program plan
In the program content development stage, an appropriate program is developed through the process of the previous three stages, and the mediation protocol or data are described. Each participant was asked to read the three classic novels, the story of Nolbu, who overeats in Heungbu and Nolbu; the story of Patji, who does not exercise in Kongji and Patji; and the story of his father, who does not take medicine properly in Shimcheongjeon, and were asked to present their thoughts on each story. In addition, the participants talked about solving problems as if they were the main characters. Finally, a game format was arranged in accordance with the traditional Korean game Yutnori for each story. The rule of Yutnori is to first throw the yut and move it by the number that came out. In the experimental group, people had to solve the quiz. If the experimental group participants get the quiz right, they can stay where they are, and if they get it wrong, they go back one step. The program content was verified by four expert nurses, two specialized in care of older people.
Step 5: Adoption and implementation plan
In practice, this is the stage of planning the application timing and execution method. This program was conducted for the elderly using the Gwangyang Health Clinic. When trying to change the subject's knowledge and attitude, it is difficult to obtain effective results through a short-term educational program (Im & Yun, 2020). Most of the studies conducted on older adults showed behavioral changes over 4 weeks, so the program was designed for a 6-week period. In addition, the small group composition, which is one of aspects of the training program, is an effective way to induce behavior change through the process of providing information for problem solving, presentation, and discussion while conducting PBL processes. A small group size of 6–8 people is most suitable (Yalom, 1985), so this program used 6–8 people. In addition, at the time of this program, group training was prohibited to prevent the spread of COVID-19 in the region, so it was conducted in small groups. The program was conducted using one novel for two weeks. The first week used a method of finding and solving problems within the story and the second week proceeded with a quiz related to this, but as a game through Yutnori.
Step 6: Evaluation plan
This is a step toward evaluating the effectiveness of the final program. This involved assessment of the value of program design and application, and any changes made after program application involving six senior citizens and their understanding of the content and difficulties related to the quiz.
Methodology
A quasi-experimental design involving a non-equivalent control group was used to verify the effect on health knowledge, health attitude, and health promotion behavior in the group to which the ST-PBL model was applied for 6 weeks. The data were analyzed using the SPSS/WIN 21.0. The general characteristics of the study subjects were averaged and converted to percentages, and the reliability of the measurement instrument was calculated using Cronbach's alpha. The Kolmogorov-Smirnov test was carried out to check whether the collected data were normally distributed, and the chi-square test and t-test were inherently homogeneous.
Instruments
1) Health knowledge: This was measured using the Aged People Health Knowledge Measurement tool developed by Ha (2004). The tool involved 10 questions, using “yes” and 1 point for correct responses; “no” for incorrect and “don't know” for unsure, both 0 points. The highest possible score was 10 points, the lowest 0.
2) Health attitudes: To measure the health attitudes of the elderly, the tool developed by Torabi et al. (2004) was modified and supplemented by the work of Yoon (2017). This tool is composed of three categories with 10 questions: health emotions (n=3), disease prevention and health lifestyle beliefs (n=3), and action intention to be healthy (n=4). A five-point Likert scale was used where “Very rarely” (1) and “Most frequently” (5). The higher the score, the more positive the health attitude.
3) Health promotion behavior: The Health Promotion Lifestyle Profile (HPLP) modified by Hong (2003) to suit the elderly was used. The HPLP tool was created by Walker, Sechrist, and Pender (1987). This tool is composed of six categories with 35 questions: nutrition (6), stress management (5), interpersonal support (6), exercise (2), health responsibility (11), and self-actualization (5). The four-point Likert scale ranged from “Very rarely” - 1 point to “Most frequently” - 4 points. The scores possible were a minimum 35 and maximum 140 points: the higher the score, the better the health promotion behavior.
Ethical considerations
This study was approved by the Cheongam University Bioethics Review Committee, Korea (No. 20-HR-013-01/CA17-190326-005-02). Survey materials with written consent forms and analysis of the data were stored in a locked file cabinet located in the principal investigator's office. Participants were informed that they could drop out at any time, without any consequences. After the end of the study, the same program was provided to the control group in consideration of an ethical response to their shared needs.
RESULTS
Verification of the Homogeneity of General Characteristics of the Subjects: As a result of testing the general characteristics of the subjects and their homogeneity, there was no statistically significant difference in the general characteristics of the subjects such as age, religion, marital status, domestic family, educational attainment, drug use, and subjective health status. It was found to be homogeneous (Table 1).
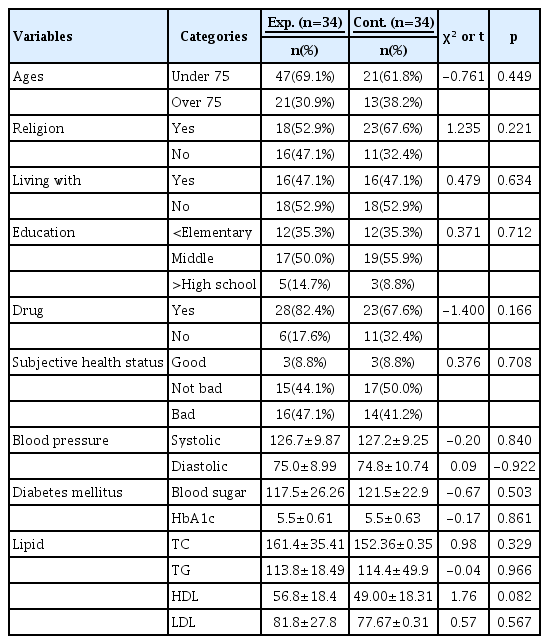
General characteristics and homogeneity test (N=68)
Verification of Homogeneity in physiological indicators: The subjects’ blood pressure (systolic and diastolic), diabetes (blood sugar, HbA1C), and cholesterol (TC, TG, HDL, and LDL) in the experimental and control groups did not show statistically significant differences (Table 2).
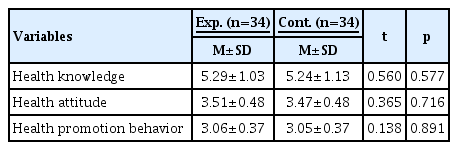
Homogeneity Test for Demographic Characteristics and Dependent Variables (N=68)
Verification of Homogeneity in Dependent Variables: The subjects’ health knowledge, health attitude, and health promotion behavior in the experimental and control groups did not show statistically significant differences (Table 2).
Verification of Hypotheses:
1) Hypothesis 1- The experimental group that participated in the ST-PBL program would have higher health knowledge scores compared to the control group that did not: Findings showed that the health knowledge score of the test group was 5.29 out of 10 before education and increased to 5.94 thereafter, after which there was a statistically significant increase (t =-3.73, p=.001). The health knowledge in the control group was 5.24 before education and 5.24 thereafter, not a significant difference (t=-1.22, p=.066). Therefore, this hypothesis is supported (Table 3).
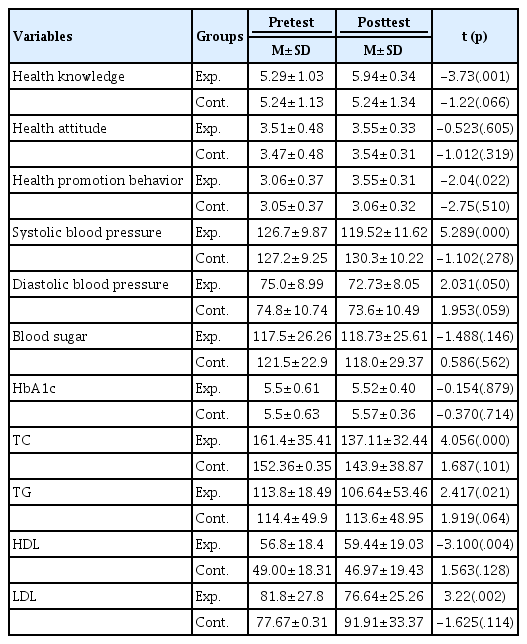
Comparison of Dependent Variables between Two Groups after Treatment
2) Hypothesis 2- The experimental group that participated in the ST-PBL program would have higher health attitude scores compared to the control group that did not. The findings showed that the health attitude score of the test group before training was 3.51 out of 5 and increased to 3.55, after training (t=-0.52, p=.605). The health attitude score of the control group was 3.47 before training and 3.23 thereafter, not statistically significant differences (t=-1.01, p=.319). This hypothesis is not supported (Table 3).
3) Hypothesis 3- The experimental group that participated in the ST-PBL program would have a higher health promotion behavior score compared to the control group that did not. The findings showed that the health promotion behavior of the test group was 3.06 out of 4 before the training and 3.55 after the training, a statistically significant increase (t=-2.04, p=.022). The health promotion behavior of the control group was 3.05 before the training and 3.06 after the training, not a statistically significant difference (t=-2.75, p=.510). This hypothesis is supported (Table 3).
Positive changes in physiological indicators: In the experimental group participating in the ST-PBL program, systolic blood pressure (t=5.289, p<.001), TC (t=4.05, p<.001), TG (t=2.417, p=.021), HDL (t=-3.10, p=.004), and LDD (t=3.22, p=.002) positively changed.
DISCUSSION
The purpose of this study was to verify the effects on health knowledge, attitudes, and health promotion behaviors by applying programs provided to the elderly with chronic diseases in rural areas, and to discuss the results.
The health knowledge score of the elderly living in rural areas improved to 5.94 out of 10 points after the program was applied, proving the effectiveness of this program. In previous studies, the health knowledge score of the elderly who lives in city was 7.51 points, and in a study by Park & June (2011) and Kim et al (2008), their score was 7.10 points, which was higher than the results from this study. Hwang (2016) study of older people in rural areas have low understanding of health-related knowledge, confirming a need for change. Existing lecture-style educational methods that simply deliver information are not suitable for older people in rural areas with relatively low understanding of health issues. Use of the classic novels facilitated exploration of health-related problems like their own, ways to solve the problems on their own, and apply new knowledge through participation in games at the end of the program. This new educational method for the rural elderly was engaging, learner centered and promoted ongoing learning through behavior change.
The results of this study showed that the health attitude scores of the experimental group did not increase significantly. As there are no previous experimental studies to improve the health attitudes of the elderly, comparisons are limited. According to Yoon (2017), the more positive the health attitude, the higher the health promotion behavior. Attitudes toward health are composed of positive emotions related to health, attitudes toward disease prevention and lifestyle, and intentions for health behavior. If they show a very high causal relationship with health promotion behaviors, a change in positive health attitudes is important. Changes in health attitudes are important because health behaviors, such as the management of hygiene related diseases, are added. First, the correct attitude change requires new knowledge (Kim & Yoon, 2012). However, positive attitude changes that can induce behavioral changes are not formed in a short period of time (Im & Yun, 2020). Since this program was applied for a short period of 6 weeks, there was a limit to our ability to confirm changes in the attitudes of the older people. Therefore, educational strategies over a longer timeframe are recommended for future education programs.
The health promotion behavior scores of the experimental group participating in this study increased significantly after the program. Previous studies have indicated that there is a correlation between health knowledge and health-promoting behavior (Kim et al, 2008,Park et al., 2018,Hwang, 2016). To maintain and improve the health of older people, it is necessary to provide continuous meaningful and relevant health management tools so that self-care can be performed. In other words, it is necessary to provide up-to-date health showcase preventive health behaviors and information about how best to live a healthy retirement. Improvements in lifestyle habits for chronic disease management are not made within a short period of time, but it is important for older people in collaboration with health professionals to make continuous efforts with patience and persistence; this will ultimately lead to behavioral change through education and counseling (Son & Song, 2007).
It is difficult for the elderly to change their behavior for self-care because of the lifelong habits, beliefs, and attitudes that have remained fixed over the years. However, most of the previous studies in Korea have applied an educational program with one topic such as nutrition, exercise, and maintenance to manage chronic diseases in the elderly. In contrast, many studies abroad have focused on lifestyle changes (Burke et al., 2005;Drevenhorn et al., 2007;Miura et al., 2004), rather than single interventions such as exercise and nutrition. To overcome the limitations of domestic research, a change in health must be brought about so that an educational program with integrated management strategies can be applied.
Results were collected on the last day of the six-week study by the lead researcher via participant surveys, BP and blood tests (table 1). The results of this study showed that in the experimental group participating in the ST-PBL educational program, systolic blood pressure, TC, and TG decreased, and HDL significantly increased compared to the control group. These results are difficult to directly compare because there are few previous studies that have applied education programs for chronically ill patients living in rural areas. The study results of Sung et al (2018) decreased in TC and TG. Also, the results of the study by Sung & Lee (2010) are like those in which TC decreased. These are the same as the result of a study in which the blood pressure of participants was reduced within a project relying on small group discussions (Zhang & Kim, 2016). Although the content of this program is different, it is true that when an appropriate educational program is provided for the elderly, a positive effect appears on physiological indicators. Therefore, it is necessary to develop and apply educational programs suitable for the elderly to bring about positive effects.
CONCLUSION
In this experimental study, the ST-PBL program was developed and applied to the elderly with chronic diseases living in rural areas. The influence of the program was evaluated in terms of health knowledge, health attitudes, and health promotion behaviors. It was demonstrated that the health knowledge and health promotion behaviors of the experimental group who participated in the ST-PBL program were enhanced. The use of elements of PBL within the educational program (use of small groups, relevant stimulus material focused on the learners’ real needs, seeking new knowledge for application to daily practice), can improve appreciation of the value of self-care skills in managing symptoms of chronic diseases.
Acknowledgements
This paper was supported by funds from the Halla•Newcastle PBL Education Research Institute in 2020.
Notes
Conflict of interest
The authors declared no conflict of interest.